Progress Report 9 (4/6/2018)
Progress Report #9:
Since our last report, we have made marked strides into creating a model that better mimics the cranial cavity in which a direct aspiration thrombectomy occurs. At our last progress report, we were left without a pump and were wondering on how to best proceed with experiments. After extensive searching, we were able to locate a pump in Dr. David Merryman’s lab. Through modifications, we were able to fit our system properly to fit the pump. The configuration can be seen below (Figure 1).

Figure 1: Pump (left) connected to fluid system.
Additionally, unlike the last pump, we could accurately mimic physiological blood flow parameters (~100 mL/min). We then decided to repeat the same experiments as we had done in the previous week to see if our results were similar. In our first experiment, we used the unoccluded state and increased the ICP in 15 mm Hg (~2 kPa) increments to see the effect on the proximal and distal locations of the occlusion (Figure 2).
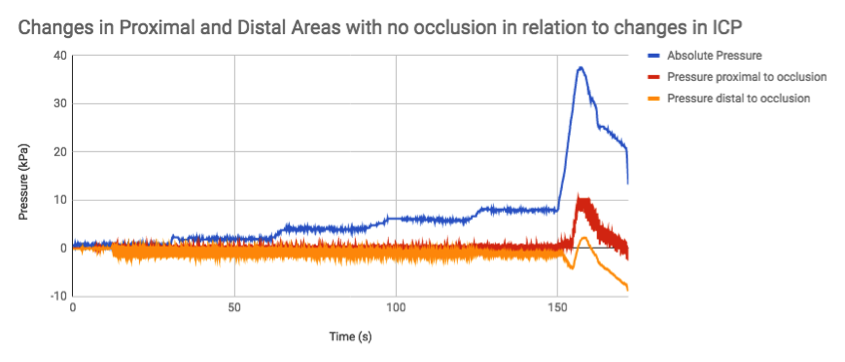
Figure 2: Increments in pressure can be seen above. Once at 60 mm Hg, the ICP was increased to maximum pressure (~150 s) to track the effect on both locations.
The results we collected were similar to our previous attempts on the other pump, as there was no real change with the proximal and distal occlusion states until an exorbitant ICP increase. Therefore, we decided to move on to the occluded state and see the pressure measurements in response to an ICP increase (Figure 3).
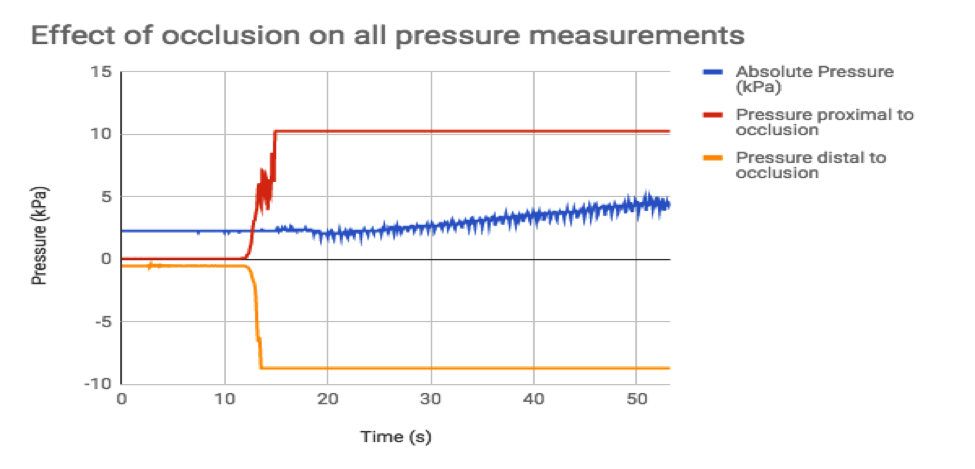
Figure 3: Pressure changes with occlusion and pump.
Instead, however, we found that the act of turning the pump on with an occlusion present was unsustainable, as both proximal and distal pressure gauges exceeded their maximum capacity, and the ICP pressure tracker began increasing without any stimuli that we added in our model. We realized that the pump was not compensating for the occlusion as the previous pump had, making it pump water regardless of the consequences. Therefore, we decided to introduce a collateral artery that would represent the capillaries present in the model, along with a one-way stopcock to provide resistance. The results are visible in the unoccluded (Figure 4) and occluded states (Figure 5).
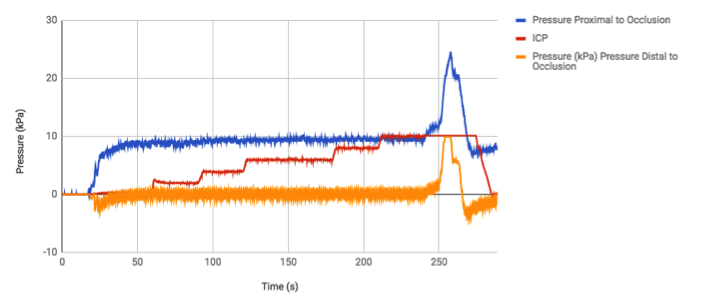
Figure 4: Response of pressures to ICP increases in the unoccluded state. The differential and absolute pressure gauges were switched to better capture the quantity of pressure increase in the proximal area as a response of unregulated ICP increase.
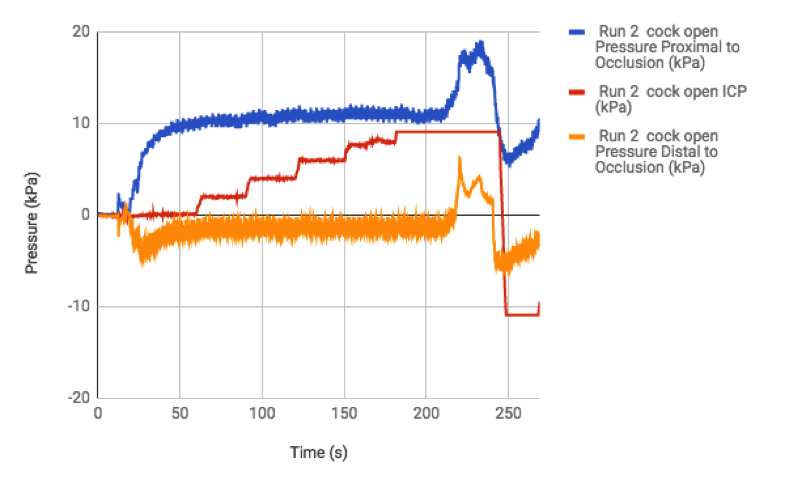
Figure 5: Response to ICP increase in occluded state.
Although we did not detect much of a reaction in the distal location, we did notice slight increases in proximal pressures as a result of ICP increments. We have not run statistical tests as of yet to try and understand if the differences are correlated, but preliminary results do show promise when concerning our original hypothesis, which did surmise a connection between ICP and pressures around a clot.
In addition to the pressure manipulation experiments, we wanted to find a material that would be more accurate in being a clot rather than a clamp. Our prime candidate was the foam used in ear plugs, but in preliminary experiments, we could not measure the suction force of our catheter with the clot, as air passed too easily through it. Fixes to this problem include getting a more sturdy material, such as rubber.
Future Plans:
- More experiments to conduct statistical analysis to definitively on the effect of ICP increase and the pressures proximal and distal to the clot.
- Use of better clot material to utilize in model and catheter suction force tests.
- Creation of Poster for Design Day.
©2026 Vanderbilt University ·
Site Development: University Web Communications