Progress Report 6 2/16/18
After adding a differential pressure gauge across the simulated occlusion, and beginning preliminary experiments on the relationships between intracranial pressure and arterial pressure, we were well on our way to creating a better optimized model to mimic direct aspiration thrombectomies. In the weeks in between the last progress report, we connected the electric pump we received from Dr. Froehler and mimicked semi-pulsatile flow in our model, and received thin-walled tubing that we hope to use in further models.
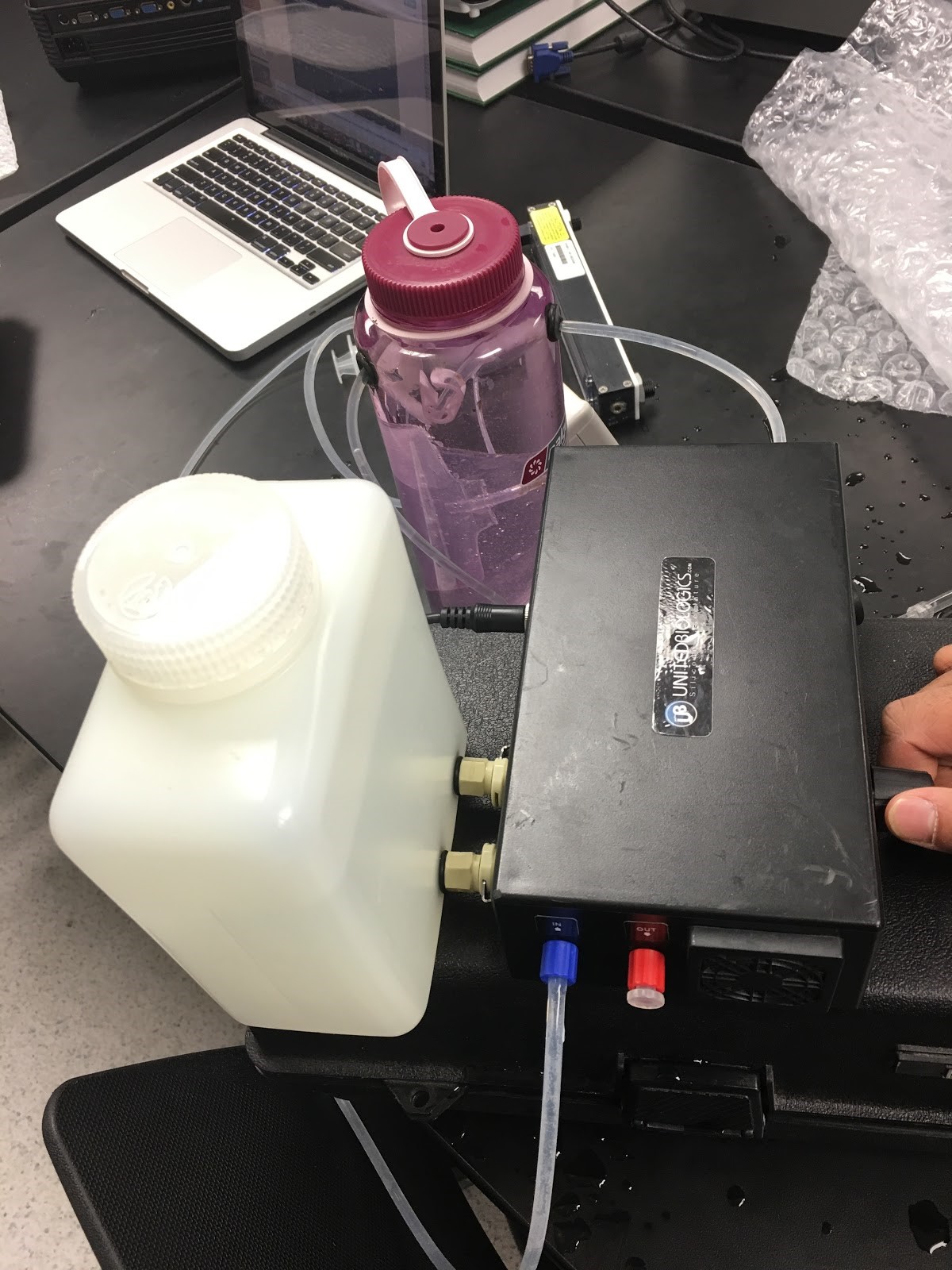
The pump we received was much more different than the prototype we had initially created, and much more efficient. A water container plugged into the device as a reservoir, and in and out ports were present to complete the water circuit. Additionally, a knob was placed to control the force of the flow throughout the tubing, allowing us to easily adjust the model if needed. Through the differential pressure gauge, we did find that the flow was indeed semi-pulsatile, but also found that, again, increasing the simulated intracranial pressure had little or no effect on the flow overall. After pondering several causes, we came to the conclusion, along with Dr. Walker and Dr. Froehler, that our model’s tubing still did not follow physiological parameters, and needed to be thinner in order for an effect to be truly present.
After presenting our progress to Dr. Walker on February 7 in the form of an oral presentation, he advised us to contact the Vanderbilt Center for Experiential Learning and Assessment (CELA), an organization that seeks “Uncompromising excellence in the education of medical professionals through human, technical, and anatomical simulation.” We suspected that they may have tubing that accurately models the cranial arteries, however upon contacting CELA, they informed us that they “do not have anything that depicts/simulates the cranial arteries.”
Moving forward, we hope to improve our model by completely sealing the model such that there are no leaks and no pressure can escape the bottle. In addition, we plan on installing the thinner silicone tubing that we received this week, and running experiments to see if this tubing more accurately represents the mechanical properties of cranial arteries. During the installation of the new tubing, we plan on including a much longer length of tubing (about 8”) inside the water bottle so that there is more arterial surface area for the elevated ICP to act on. Additionally, we plan on adding a one-way stopcock that will model the resistance of the capillary bed in the brain vasculature. This valve will be placed outside of the model and be mostly closed to simulate the vast pressure drop across the capillaries.
Finally, we intend to investigate the effect of increased ICP on the vacuum pressure that can be pulled at the tip of the catheter. We will do this by placing a negative pressure gauge hooked up to the tip of the catheter inside a closed and pressurized compartment, and measuring the pressure at the tip of the catheter under various different intracranial pressures.
©2026 Vanderbilt University ·
Site Development: University Web Communications