
Definition of the Term and Background
Abstinence-only sexual education programs are programs that meet the 8-point federal definition of “abstinence education” as established in the 1996 Welfare Reform Act (Ballaro & Ginsburg 2016). These programs have the exclusive purpose to teach the “social, physiological and health gains to be realized by abstaining from sexual activity,” and that a “monogamous relationship in the context of marriage” is the expected standard for human sexual activity (Ballaro & Ginsburg 2016). Such programs also require teaching that sexual activity outside of marriage is likely to have “harmful psychological and physical effects,” (Ballaro & Ginsburg 2016). The programs are allowed to mention contraception options only in the context of failure rates (Wiley 2002). Titles of such programs that meet this federal definition and receive funding include Choosing the Best Life, Friends First, and Managing Pressures Before Marriage, indicating these programs include lifestyle advice in addition to information on sexuality (U.S. House of Representatives 2004).
Abstinence-only programs stand in contrast to comprehensive sexual education programs. Comprehensive programs, sometimes referred to as “abstinence-plus” programs, emphasize the benefits of abstinence while also teaching about contraceptive methods and sexually transmitted disease (STD) prevention (Ballaro & Ginsburg 2016). Zero comprehensive sexual education programs receive federal funding (Wiley 2002).
In the United States, 39 states have a mandate to teach sex education in public secondary schools (Sex and HIV Education 2017). Of these 39 states, 26 require this education is taught using abstinence-only curricula. For example, Madison County in Mississippi has a state mandate to teach abstinence-only sexual education and uses Choosing the Best Life series of textbooks to do so (U.S. House of Representatives 2004). An analysis on the Choosing the Best Life program and other similar program is discussed below. Image 1 shows a map with states in which information on abstinence (and not contraception) must be provided during sex education. The group of states with such mandates includes Arkansas, Oklahoma, Mississippi, and Texas, which are the four states with the highest adolescent pregnancy rates in the United States (Health and Human Services 2017). Taxpayers in Texas alone pay approximately $1 billion annually for costs relating to teen childbearing (Wilson 2009). A case study in the state of Texas revealed that 94% of Texas public school students receive no sexual education apart from the promotion of abstinence and that a small number of districts ignore the mandate to teach sexual education altogether (Wilson 2009).
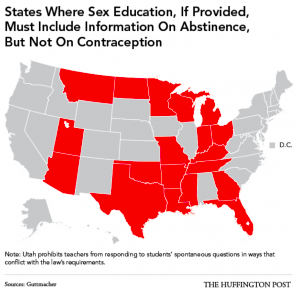
Image 1: “States Where Sex Education, If Provided, Must Include Information on Abstinence, But Not on Contraception,” (O’Neill et al. 2016). This map shows that many states in the south and mid-west mandate that information on abstinence must be provided during sexual education, but not information on contraception.
The Welfare Reform Act of 1996 first established federal funding for abstinence-only programs. Such programs receive $50 million annually, with states matching $3 million for every $4 million received (Wiley 2002). A selection of 13 of the most popular abstinence-only curricula for public schools was reviewed for scientific accuracy by the United States House of Representatives Committee on Government Reform was prepared in 2004 for Representative Henry A. Waxman (U.S. House of Representatives 2004). The report found that over 80% of curricula that received federal funds contained “false, misleading or distorted information about reproductive health.” Erroneous claims regard effectiveness of contraceptives, risks of abortion, and biological processes. One program reported that “pregnancy occurs one out of every 7 times that couples use condoms” while another stated that “abortion leads to an increased risk of mental retardation in following births,” (U.S. House of Representatives 2004). The program Why kNOw falsely stated that 24 chromosomes from the mother and father join to create a new individual, while the correct number is 23 (U.S. House of Representatives 2004). Other programs treat stereotypes about girls and boys as fact, sharing that women need “financial support” while men need “admiration,” (U.S. House of Representatives 2004). These statements undermine female achievement and imply that females are dependent on males for protection.
Another review of abstinence-only curricula in Texas had similar findings. This review found that Texas programs are presenting “worst case scenarios” to scare students, include shaming messages that sex is “dirty and immoral” and that virgins are “better” than people who have had sex, and are mixing religious messages with sexuality education (Wiley 2009). Though there is debate over whether or not abstinence-only programs should continue to be used in public schools, the empirical evidence is undeniable. The United States has the highest adolescent pregnancy rate out of any industrialized country, with 3x the rate of France and 5x the rate of the Netherlands (Ballaro & Ginsburg 2016).
Historical context
Abstinence from sexual activity (be it lifelong or until marriage) is rooted in religion (Gresle-Favier 2009). For centuries, Catholicism has preached that sexuality is sinful and draws believers away from God. In 17th and 18th century England, social critics equated premarital sex to “disorder and immortality,” (Godbeer 2002, 36). Colonial historians argue that Puritan settlers brought these concerns and criticisms about sexuality to the New World. Abstinence from sexual activity until marriage was fundamental in the lives of the forefathers of the United States, as there was no reliable contraception at the time. The virginity of the bride was also imperative to “guarantee legitimacy of the husband’s offspring,” (Gresle-Favier 2009, 7). However, as population size increased and the saloon culture took hold of the growing nation, abstinence until marriage became less of a priority for many Americans.
It was not until 1904 that psychologist G. Stanley Hall conceptualized “adolescence” as a separate period of life distinct from adulthood (Gresle-Favier 2009). Hall believed this period of youth had to be characterized by chastity to ensure proper development of virtue and character. His pro-abstinence sentiments were echoed by social hygienists in the early 1900s in their campaign against venereal diseases and prostitution (Gresle-Favier 2009). These social hygienists felt that if children were educated scientifically about the risks of sexual activity, the children would make healthy choices and remain abstinent until marriage. They proposed bringing sex education to schools as early as 1910 (Gresle-Favier 2009). However, these proposals were met with strict opposition by conservative Christian groups who believed the inherent innocence of children would be corrupted by such education (Gresle-Favier 2009).
The United States witnessed an unprecedented rate of venereal disease following World War One (1914-1918), first in the military and soon after in the civilian population (Gresle-Favier 2009). At this time, anti-sexual education advocates began to shift their perspective, determining that the modern world was already corrupting children and that it was best for information regarding sexual activity to come from a reliable, moral source. Information about abstinence and the risks of sexual behavior were taught at community centers, health centers, and even churches (Gresle-Favier 2009). By 1964, proponents of abstinence formed the Sexuality Information and Education Council of the United States (SIECUS) with the objective of making information on sexuality widely available (Gresle-Favier 2009). While it was criticized for encouraging promiscuity, the information was still heavily imbued with risks, warnings and moralistic messages. In 1968, a religious group called the Christian Crusade” ran a newspaper ad featured below (Image 2).
Image 2: “Is the School House the Proper Place to Teach Raw Sex?” (Davis & Frank 2016). This image circulated in a 1968 newspaper encouraging state and local governments to restrict sexual education in public schools.
The 1970s sexual revolution saw more Americans than ever before supporting premarital sex. Marriage was “losing its privileged position as the sole site for sexual relations,” (Gresle-Favier 2009, 10). While the liberal left argued that contraception and abortion needed to be readily available to protect young women from teen pregnancy, conservatives felt the problem was not the lack of resources, but sex itself (Gresle-Favier 2009). They continued to push abstinence from a moral angle. However, the 1980s AIDS epidemic confirmed that the need for sexual education in schools could no longer be ignored. Thus, a new strategy was developed, and the designing of abstinence-only curricula for public schools began (Gresle-Favier 2009). Conservative Christian groups pointed out that “God had conveniently arranged life so that morality and hygiene were indistinguishable,”(Gresle-Favier 2009, 12).
Federal funding for abstinence-only sexual education began under the Reagan administration and skyrocketed during the George W. Bush administration (United States House of Representatives 2004). Between the years of 1996 and 2007, the US Congress committed over $1.5 billion (through both federal and state matching funds) to abstinence-only programs (Ballaro & Ginsburg 2016). This funding reflects a sustained commitment to abstinence-only education by the federal government. The same anti-sexuality sentiments present in the Puritan settlers continues to keep its hold today in public school sexual education.
Perspectives
Though the debate on whether or not to discuss sexuality education in public schools has been settled for decades, the debate of what type of sexuality program to use remains a hot topic. Abstinence-only advocates say their approach provides young people with the information they need to arrive at the “healthiest possible outcomes,” (Ballaro & Ginsburg 2016). They feel comprehensive programs may give teens a false sense of security in believing condoms are a fool-proof form of pregnancy and STD prevention, and that this mindset may lead to increased promiscuity. Proponents point to statistics that show a drop in teen pregnancies in years during which these programs have been in place (Ballaro & Ginsburg 2016). When presented with the 2007 congressional study that demonstrated shortcomings in abstinence-only education programs, the Associate Commissioner of the Health and Human Services Department, Harry Wilson, said that the study was not rigorous enough to reveal whether or not abstinence-only programs work to reduce adolescent pregnancy and STD rates (Gresle-Favier 2009). However, it is important to note that the goal of these programs is not solely to reduce the aforementioned rates. It is to curve the sexual behavior and ideology of America’s youth. This discussion is continued under the “Politics of Health” heading.
Opponents of abstinence-only sexuality education programs say that these programs are responsible for the epidemic of STDs among young people (Ballaro & Ginsburg 2016). They assert that such programs are promoting ideology and politics instead of scientific evidence. Opponents feel abstinence-only programs deny the realities of contemporary society and of adolescent sexuality, drawing attention to the statistic that 70% of 18-year-olds have engaged in sexual activity (Ballaro & Ginsburg 2016). Further research suggests that comprehensive sexual education programs lead to “neither earlier or increased sexual activity” and that teens are more likely to use contraceptives and seek STD screening when they do begin to have sex (Ballaro & Ginsburg 2016). Finally, opponents view federally funded abstinence-only sexual education programs as a form of censorship with “deadly consequences,” as more than half of all new HIV infections occur under the age of 25 (Ballaro & Ginsburg 2016). Today, 18 states and the District of Columbia require that scientifically accurate information about contraceptives be taught in sexual education programs (Sex and HIV Education 2017).
Recently, LGBTQ advocate groups have advocated for more inclusive curricula being designed to target America’s cis and LGBTQ youth alike. More information on the topic can be found here: http://teenhealthsource.com/blog/queering-sexual-education/.
Relation to Politics of Health
Abstinence-only sexual education is related to politics of health because it is a form of biopower (Foucault 1978). The term biopower was coined by Michel Foucault and refers to the subjugation of bodies to control a population. Given abstinence-only sexual education programs are federally funded and comprehensive sexual education programs are not, the state is taking a clear stance on expected sexual behavior. However, as discussed by author Alexander McKay, the debate over sexual education programs is “not simply a dispute over the most effective means to promote sexual and reproductive health of youth,” but is “a clash over the shape and direction of society itself,” (Gresle-Favier 2009, xiii). The funding of abstinence-only sexual education programs enables conservative ideologists and administration in power to control bodies (both psychologically and physically) as a means to preserve traditional hierarchies. McKay asserts that beliefs on sexuality are important in that their organization “significantly shapes the nature of society,” (Gresle-Favier 2009, xii). Therefore, the debate over sexual education is heightened, as it is an instrument to socialize America’s youth and set the values and behavioral norms of society. At its core, it is not a discussion about reducing adolescent pregnancy and STD risk, but a battle over a wider social conflict about sexuality and ideologies in America.
« Back to Glossary Index