
On April 26th, 1986, the Chernobyl Nuclear Power Plant experienced a power surge which led to the destruction of one of the plant’s nuclear reactors, Chernobyl 4. The meltdown, caused by a combination of a flawed reactor design and human error, resulted in a fire which lasted ten days and released lethal amounts of radiation into the air. As a result, two people died on sight and 28 people died within the first four months after the accident from radiation poisoning (“Facts Sheet” 2017). Chernobyl was originally regarded as in Russia until years later when Ukraine, where Chernobyl is now considered to be located, won its independence from Russia. Russia felt that it had very few obligations to its citizens after the plant meltdown; its government limited resettlement actions and investigations of the effects of radiation exposure. While this original attitude by the Russian government led to many more people becoming ill due to radiation exposure, the Russian government had very specific criteria for labeling these people as sick, thus preventing many from receiving care. However, when Ukraine won its independence, its government lowered the criteria for being considered sick and expanded the exposure radius to include people who lived farther away, increasing state recognition of illness cause by the Chernobyl disaster (Petryna 2004). Chernobyl was the only historical incident of a commercial nuclear power plant causing fatalities from radiation, which could be because the Chernobyl plant lacked the safety mechanisms that nuclear power plants worldwide are legally required to have. Because of the lack of safety measures, after the incident, a concrete sarcophagus was built around the reactor to prevent future leaks, however, this device was deemed structurally unsound and inadequate to protect against future radiation damage, causing the government to force a more widespread evacuation of the area (“Facts Sheet” 2017).
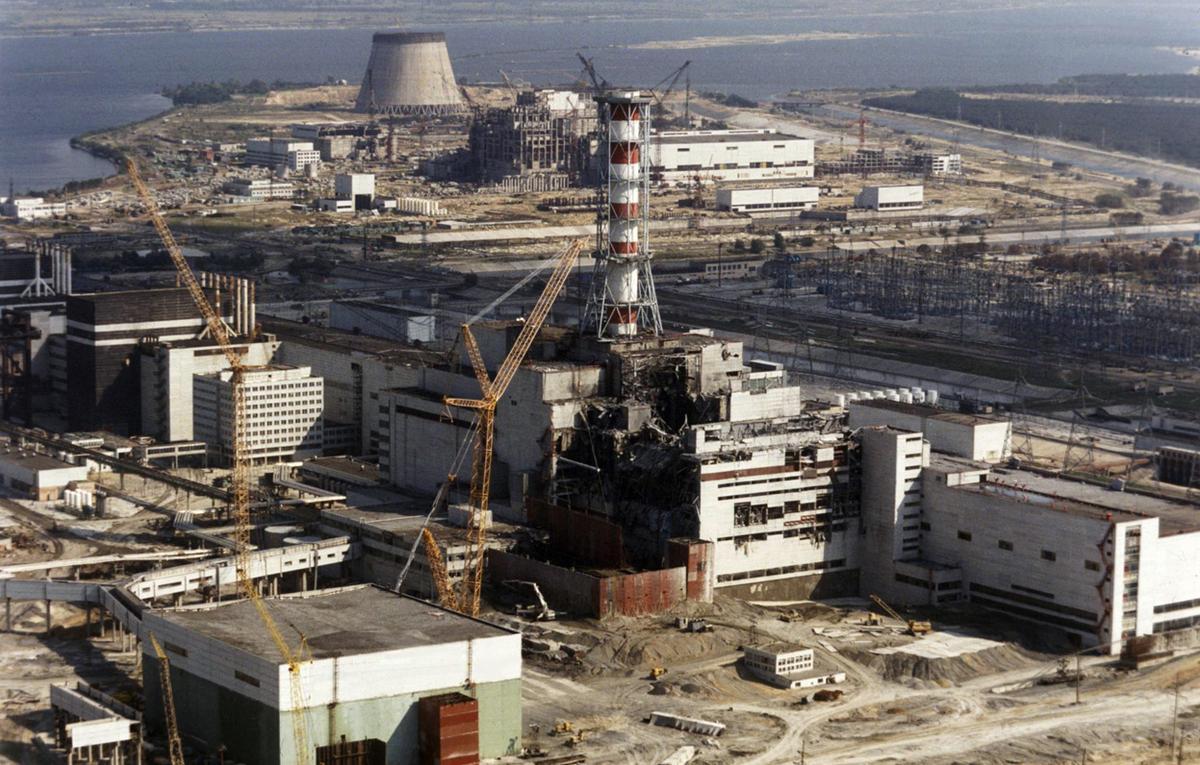
Chernobyl 4 after the reactor melted down
The lack of these safety mechanisms was the reason that the ramifications from the meltdown were so widespread and grave. To put the incident in context, the Chernobyl plant lacked every required safety mechanism and every preventative safety policy that the US employed at the time to mediate the risk of radiation exposure. After a partial meltdown at the Three Mile Island nuclear power plant in 1979, seven years prior to Chernobyl, the United States significantly revamped its policies and safety procedures regarding nuclear power. Before the meltdown at Three Mile Island, the US still had very strict guidelines for equipment and crisis management at nuclear power plants. Thus, the Three Mile Island incident did not yield any negative health effects, like the Chernobyl meltdown did. After Three Mile Island, the US instated over 20 changes to nuclear power policies to ensure flawless plant designs, reduce human error, and enhance emergency preparedness to mitigate long term health effects in the case of exposure (“Backgrounder” 2017). Of these revisions, the two most notable of these policy changes that were lacking in Chernobyl were those of alert and notification and protecting the food chain. The plant operators at Chernobyl attempted to cover up the accident and refrained from telling authorities and locals about the radiation leak until 36 hours after the reactor malfunctioned. However, in the US, nuclear power plants are required to alert authorities and make recommendations for protecting the pubic within 15 minutes of a suspected nuclear release (“Facts Sheet” 2017). This discrepancy in timing allowed ample opportunity for the surrounding population to be exposed to large amounts of radiation before they were aware of the problem and given the chance to evacuate. Similarly, because of the initial cover up of Chernobyl, many people unknowingly consumed contaminated milk and food. In the US, federal regulations mandate a close monitoring of local livestock and water after exposure in order to mitigate any risk and stop the spread of contaminated foods. Because of these two regulatory flaws, many more people were exposed to radiation, thus causing the ramifications of the incident to be more severe and widespread than if safety precautions would have been implemented (“Facts Sheet” 2017).
However, determining the specific health consequences of the Chernobyl incident is a highly controversial subject. Many experts have differing opinions on the exact levels of radiation exposure that the accident caused. Because the effects of chronic exposure to low doses of radiation were relatively unexplored before Chernobyl, most of the research done on the topic was conducted retrospectively, making it harder to generalize the data and use it to estimate the effects of Chernobyl. However, there was some research on the topic from the nuclear bombings on Japan. These studies found that most of the detrimental long-term effects of radiation exposure were not seen in the population until 25 years after the initial incident (Paris 2006). With Chernobyl being just 30 years ago, it is difficult for researchers to reach a consensus of the number of people affected, as the number is still growing as the years pass. Another controversy surrounding the health impacts of Chernobyl is accounting for the risk of thyroid cancer. Shortly after the incident, researchers believed that the population had only been exposed to iodine-131, an isotope that had not before been explicitly linked to cancer. However, it was later discovered that those around Chernobyl were chronically exposed to many more shorter-lived iodine radioisotopes through both internal and external measures. This type of isotope combined with the intense, long-term exposure was much more likely to cause thyroid cancer. This confusion over the type of exposure led many scientists to disagree on the impact of the radiation and to severely underestimate the levels of thyroid cancer that would result from this incident (Paris 2006).
The connection between the Chernobyl disaster and politics of health is best seen when discussing these high levels of infection that could have been prevented by simple policy changes. One of the biggest political issues with the Chernobyl disaster was that the government violated its most basic duty to its citizens by failing to protect them from and compensate them for this irreparable harm. In the immediate years after the accident, the local hospitals were not provided with adequate funds from the government to purchase enough equipment, drugs, or food to effectively serve the affected population. The present-day Ukrainian government is even still struggling to provide sufficient healthcare and housing for those affected by Chernobyl and has not taken steps to alter legislation to make this process easier and more feasible (Anisimov and Ryzhenkov 2016, 267). This exclusive nature of providing care fostered by limited resources has led to health professionals using their sympathies to award state recognition. This process of sympathy and exclusion has been propagated by the government policies which dictate who is ‘sick enough’ to achieve access to resources. As evidenced in Petryna’s piece, doctors have the ability to hand pick whom they deem worthy of treatment by asking leading questions to amplify the extremity of individual’s illnesses, thus making the process of awarding resources more subjective and liable to individual biases. This relates to Petryna’s idea of biological citizenship being tied to citizens needing to utilize an illness to receive adequate attention and care from their government (Petryna 2004, 261). The concept of biological citizenship focuses on using claims of illness to compete for scare government resources, which was seen after the Chernobyl disaster. Because there are such strict regulations about access to care, the need for already scare resources and recognition has become even more competitive. These people who have been affected by the Chernobyl disaster have had to use their illness as a way to promote themselves and achieve certain basic right of healthcare instead of as a detriment like most sicknesses are seen (Petryna 2004). The biological citizenship propagated by the Chernobyl incident forced individuals to utilize being sick to their advantage to gain attention, when they as a sick population, should have been a priority no matter level of illness or scarcity of resources. Because healthcare resources are so scarce, receiving proper medical care has become a highly politicized issue that involves playing on ones own weaknesses to elicit sympathy and support from the government. This relation further proves that individual rights, in this case medical care, can be infringed upon because of the government’s misallocation of resources. While healthcare should ideally be separated from politics, the two are so interdependent that citizens have to use their medical conditions to compete against each other for resources.
References
Anisimov, Aleksey Pavlovich and Anatoliy Jakovlevich Ryzhenkov. “Thirty Years After the Accident at the Chernobyl Nuclear Power Plant: Historical Causes, Lessons and Legal Effects.” Journal of Energy & Natural Resources Law 34, no. 3 (08, 2016): 265-283. doi:. http://login.proxy.library.vanderbilt.edu/login?url=https://search-proquest-com.proxy.library.vanderbilt.edu/docview/1851053498?accountid=14816.
“Backgrounder on the Three Mile Island Accident.” United States Nuclear Regulatory Commission – Protecting People and the Environment. Accessed April 02, 2017. https://www.nrc.gov/reading-rm/doc-collections/fact-sheets/3mile-isle.html.
“Fact Sheets.” Chernobyl Accident And Its Consequences – Nuclear Energy Institute. Accessed February 20, 2017. https://www.nei.org/Master-Document-Folder/Backgrounders/Fact-Sheets/Chernobyl-Accident-And-Its-Consequences.
Paris, Ann MacLachlan,. “French experts: Precise effects of Chernobyl will never be known.” Nucleonics Week. November 23, 2006 . Date Accessed: 2017/02/20. www.lexisnexis.com/hottopics/lnacademic.
Petryna, Adriana. “Biological Citizenship: The Science and Politics of Chernobyl-Exposed Populations.” Osiris 19 (2004): 250-65. doi:10.1086/649405.
« Back to Glossary Index